If you think you may have bust your tendon, or at the very least you’re injured / can’t walk properly:
< Stop reading and get to the ER straight away to get medical attention!! >
Time is now of the essence, it really will make a positive difference later on;
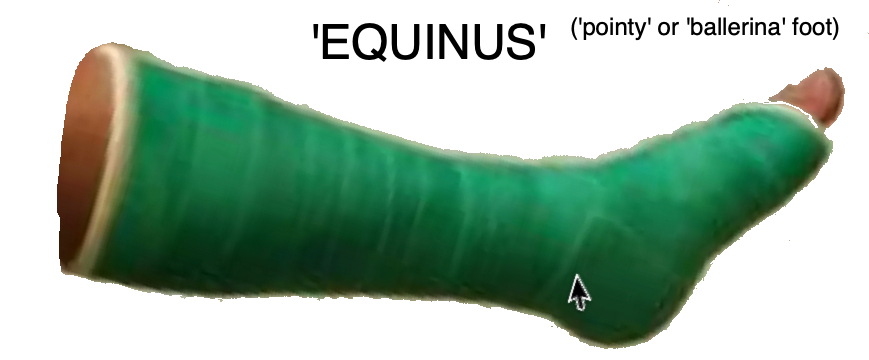
DON’T walk on your injured leg – keep it ‘pointed like a ballet dancer’;
once you’re safely in the ER and waiting for a doc / scans / etc.,
you’ll have time to read on … I hope at least some of what I’ve written will help!
Regardless, of whether there is going to be an operation or not: for the shortest recovery time and maximum return to full functionality, it’s important to act swiftly in that first post-injury moment. Not that there is a guarantee for either, but the longer it takes (with possibly stepping around on and causing further damage / hindering the short-term healing), the harder the rest of the road to recovery is going to be.
So, the first things to happen to me, which were all done in the ER hospital inside a couple of hours (at no cost to me – I am sooo grateful for the German health system 🙏):
- ‘Thompson Test‘: typically done whilst lying on your front with the feet hanging over the bottom end of the hospital bed; doctor will squeeze your ‘good’ calf, the foot should move / twitch ; same squeeze on your injured side calf, the ‘bad’ foot doesn’t move = full rupture;
- Ultrasound (echocardiography): this is not terribly precise for this kind of injury (contrast between tendons and fluids is not high, resolution same), but if both the operator and machine are good, it is a quick and cheap way of getting a reasonable internal picture … certainly way quicker and cheaper than an MRI!
- X-ray: my initial reaction was like, “Huh? But you can’t see soft tissue on an x-ray!” … which is true, but they’re doing it to make sure that there really is neither a fracture nor bone splinters floating about;
- Boot fitting (you may get a cast at first before getting a boot): once the docs had ‘done their thing’, a nurse came and fitted me with a VACOped boot – apparently this is not so well known in the US, where there are lots of cheaper and (in my opinion) less-suitable ‘tools’ for the job; a cast initially also seems to be common elswehere … but I’m pretty sure that a cast is completely unnecessary if you get this boot. And I’m lucky enough to live literally just down the road from the global headquarters of Oped (website in English / Deutsch), the manufacturer of this boot, so it gets used here as standard ‘prescription’ healing equipment. I would insist on exactly this boot, knowing what I do now – if I had to pay a thousand bucks myself and I had that option, I would nevertheless do it in the blink of an eye (last time I looked, it’s on Amazon for under 300$);
- Anti-coagulant injection (aka blood thinner; for me in the form of Clexane single-use injections): GP confirmed yesterday (almost 4 week mark for me) that I should continue injecting myself daily until I am no longer regularly wearing the boot – whether going down a surgical or non-operative path, this is one of the most important things as DVT (Deep Vein Thrombosis) can be lethal and is a REALLY significant risk factor. I asked the question as I had thought I may be able to stop a little earlier, like at FWB (Full Weight Bearing), buuut she said no … who cares, the injections are small, don’t hurt and are easy to do yourself with zero previous knowledge and without any kind special equipment – they’re single-use disposable ones;
- Supplied with crutches: in Germany, one tends to get forearm ones; in the US, I think, underarm ones. Either way, it’s important they’re set to the right height! There will be some small ‘room for maneouvre’, it’s in any case not immediately life-critical … but the initial setting for me was definitely too low. A caregiver at a later visit to another Munich clinic noticed how hunched over I was (I hadn’t noticed!) and popped them up two notches; later, a well-meaning (but mistaken) guy at a medical services shop suggested putting them up another notch, which I did; I saw a physiotherapist (PT) a week later and he said, nope, definitely wants to go back down a notch. HE was right … having the comparison of walking around for some days each on a) way too low, b) just right and c) a bit too high, I can say it really helps to avoid back, hip and other pains to have the crutches adjusted right.
After that, it’s probably time to head home, certainly there was no question of me staying overnight … though put in this position, I certainly wouldn’t try and drive home! Nope … call for help and get a ride home, a taxi if necessary; get looked after and have a flask of water next to the bed and then try and get some rest.
If one is lucky enough to get kitted out with a VACOped off the bat, particularly in comparison to having a cast, it can, of course, be adjusted via the 4 velcro straps: if it’s pressing at any point, these can be relaxed here or there a little, shift the plastic a bit until it gets comfortable – mine doesn’t disturb me in the slightest, although I once had a pressure point after I’d showered the first time and re-applied the shoe slightly off … not dangerous, just slightly uncomfortable and at any rate, easy to correct.
Whatever you do: DON’T take the boot off at night!
(just yet)
What’s next? The next few days will be decisive; the first and (initially) biggest question will generally be does one want / can one get the ruptured tendon conservatively treated (no operation) or is there the need / desire to have an operation? BUT: if this is the day of the injury, and you have either a cast in ‘equinus’ position or a boot to provide the same, please sleep easy in the knowledge that literally everything important that can be done on the first day has already been done. The rest takes time, it’s a long process, but, barring an operation, at least it’s generally not painful once the initial swelling has ebbed … I, personally, didn’t even get close to wanting to take a painkiller AT ANY STAGE.
If an operation ends up seeming to be the best way forward (for whatever reason): it typically won’t be performed until between a few days to a week or so after the injury, depending upon the situation. So, if you find yourself lying in bed after having a shitty day finished off with a visit to the ER: do your best to get a good night’s sleep … this is really the best thing you can do at the moment.
If you can’t sleep and ‘need’ to google – well, I understand, that’s what I did: the internet is huge, and it’s a bit like asking 5 dentists how your teeth look … you’ll get minimum 7 different opinions. Hence I’ve tried to collate some information, putting it – roughly speaking – in order of relevance / priority.
Again, please realise, I’m neither a doctor nor a physio therapist … just a person who was given next to no information, despite a good initial ER treatment, who is now writing a journal, as much for my own sake (in case I re-rupture or rupture the other tendon in the future!) as for anyone else’s. Really, the best thing you can do is educate yourself and recognise that:
It’s your body … your injury … your decision.
(not any doctor’s, and certainly not mine!)
(oh yes: get a MINIMUM of a SECOND medical opinion, ALWAYS!)
< what next … ?! / urgent short-term resources – my suggestion for the next page to read >
